Corrective Breast Surgery
Not every cosmetic breast surgery is simply about being larger, smaller, or looking younger. For some women, plastic surgery can correct serious breast asymmetry or abnormality and truly change their lives.
Tuberous or Tubular Breast Deformity
Tuberous breast deformity can be one of the most challenging anomalies for a plastic surgeon to correct. Roughly 5% of all breast augmentation patients have a condition known as “hypoplastic tubular breast” or underdeveloped breasts. Many patients don’t even know they have this condition, they just think their breasts look weird and don’t know there is
According to the American Society for Aesthetic Plastic Surgery, 10% of breast augmentations surgeries on women under 18 in 2006 were for to correct tubular breasts. This condition requires the surgeon to be specially trained in the repair of this abnormality. It often can require performing a breast lift in conjunction with repositioning the displaced tissue and also adding breast implants.
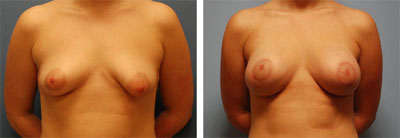
This 21-year-old patient underwent a bilateral breast augmentation and left breast mastopexy to correct a tubular breast deformity. The results were fantastic.
Breast Asymmetry
Although everyone has some degree of asymmetry between each breast, for some women it is severe. Asymmetrical breasts are a congenital anomaly that can be easily corrected with a breast implant. The degree of asymmetry doesn’t matter; if the patient is disturbed about it, she should consider correction. In some cases, it is the rib beneath that is causing the asymmetry. This condition can also be corrected with a breast implant.
Breast asymmetry can either be corrected by making one breast smaller, or one breast larger. Patients who experience this condition usually prefer one or the other, and the surgery is tailored to match the preferred breast.
Nipple or Areola Reduction Surgery
For some women, nipple reduction is sometimes the only goal of cosmetic breast surgery, but it can also be a part of a breast lift or reduction surgery. There is no ideal areola size, rather it is determined by breast size, chest size, and overall aesthetic preference. Surgery to reduce the size of the nipple or areola does leave scars, but they can be camouflaged well, and for most women who are concerned about these issues, a scar is a welcome tradeoff.
Correction of Inverted Nipples
Nipple inversion, where one or both of the nipples point inward instead of out, is actually quite common. An inverted nipple isn’t a health risk, but is a cosmetic problem that can be easily corrected. Most often this condition affects young women during breast development, or more rarely as an unwanted side effect of breastfeeding. There are varying degrees of inversion, and the severity of the inversion dictates which procedure can correct it.
3 Grades of Inverted Nipple Severity
Grade I: the inverted nipple can be pulled out and stays there without traction for a long time. It is possible to treat Grade I inversion with a suction device or a short-term nipple piercing. If these non-surgical methods don’t work, a simple purse-string suture around the base of the nipple can resolve it with no division of the milk ducts.
Grade II: the inverted nipple is more difficult to pull out and tends to retract. The ducts are shortened and there is some fibrosis. Surgery is usually required to divide the fibrous tissue, but the milk ducts can be preserved.
Grade III: the most severe inversion, because the nipple cannot be pulled out. There is a high degree of fibrosis, and the milk ducts are retracted and very short. There is a deficiency of soft tissue underneath the nipple, and surgery is required to divide all of the fibrous tethering tissue including the milk ducts. Surgery is required to correct this level of severity. The patient won’t be able to breastfeed and may lose nipple sensation.
Additional scientific information
The Inverted Nipple: Its Grading and Surgical Correction, Plastic and Reconstructive Surgery, Han S, Hong YG, 2000
The classification of inverted nipples, Plastic and Reconstructive Surgery, Scholten E, 2000

